Tag: physical therapy

Step Down Pt.2 – for knee rehab and glute strength | Feat. Tim Keeley | No.69 | Physio REHAB
admin123 0 Comments Back Pain CHRONIC PAIN
All title today we 39, re doing the step down part two now this. Is taking into account all the stages from regression right through to stepping down the BOSU and it’s, one of my favorites for knee rehab, good rehab knee ache, so let’s start off with a few cases fundamentals with the steps down. Remember it’s like a one legged hunker, but what we’re trying to do is control the e centric phase of steps down off the box, but not putting weight through the back leg. So we’re going to keep heavines on the breast leg and then stepping back up now, when you start off this exercise, some people that have knee agony or they’re just out of surgery or they’ve, got a little bit of weakness through The VMO a lot of weakness through the glutes, so we have to try and change the practice to accommodate that first things. First, what you’re going to make sure of whenever you’re doing the steps down, is your knee? The middle of your knee needs to the other, the middle of your foot. Now the midriff of your foot is between your second and third toe so that’s on the outside your big-hearted toe. So the best thing to think about is when you’re doing a steps down, think about the knee on the outside of your big-hearted toe. Alright, so you should always be able to see your big-hearted toe now. The other thing so that’s that’s hinder that in line and that’ll teach you not to go your nin, because if your knees rolling in you ,’ ll see it cross over your large-scale toe. So you always got to try and keep it out, and sometimes it goes in as a matter of. Is it my lateral rotators that a week here, as are my glutes, that a few weeks here, it’s not definitely a week VMO that moves it in that’s usually up the top now and the trendy okay, so knee adjustment is important. The hip alignment is really important as well. So when you start off you ,’ ve got to have your trendies, as in the ASIS on either side the level of the pelvis it’s got to be level. At least I’d. Preferably, it be a little bit higher on the opposite side, then you really know that you’re using your glute on this side. Your glue, meat and men. Now there you’re walking muscles. So you imagine I’m walking I’m going upstairs or I’m running that statu there. I need these muscles to keep my hip high-pitched, so I are truly clear my leg through the anchor that’s why we’ve got them all right. So when I’m walking, if I don’t know place my sky, I’ll scuff my paw, so it’s a good way to think about. Can I preserve my pelvis high to clear my leg through the soil and this position needs to be held the entire term when I’m going through that steps down that reverse doodly-squat? So if I was down here and I sag you’ll appreciate, my leg comes in a little bit. So if you’re using a mirror in front of you, you should ever see your legs parallel and not slam in that way. Let that leg droop, because you then, if that happens, you know your leg is descent. Your pelvis was putting down. So what I mean is, if I’m here, you don’t want to be throw. That nature. When I go into a diddly-squat – and you see this a lot when people doing strengthened in or step downs winding it squats, they’re flatten their pelvis. Now, if you stop your pelvis okay, you’re not doing any is currently working on your glute and then the femur is going to internally rotate what it’s going to drop into valgus, which is going to give you their knee agony, which is what we’Re trying to avoid in the first place so very important that you save that pelvis stage all right throughout the entire movement. Now one thing that can realize you quit your pelvis is, if “youre trying” reach for the field, okay, because some people run out of range in the trendy, so they’ll squatting down, they’ll run out of range now and then they’ll. Just drop alright, so you’re going to make sure that you actually bend at the hip to do the movement and sometimes they can do it because they’ve got frailties. So let’s is the beginning with the first step. We, like the regression grade and this two things. The regression of a1 is a toe tap step down, and one is a regression step down now. The toe tap step down is going into a position where you’re, actually sitting back, but you’re , not letting your knees come forward. Okay. So if you look at, if you come in here when you have a look at us, so when I stand on one leg, when I sit down to the position, be seen to what extent my knee remains relatively, where it is, I’m not letting my knee come forward. Like a ordinary steps down, I’m just prevent it there and sitting backwards now from there. I’ve got to try and are of the view that static situate. Okay, tap my paw on the back, tap it on the front and the heel tap it on the back. So I’m not actually moving on my heavines bearing leg. I’m trying to hold this isometric contraction of my knee my quad here my hammy, my glute saving my pelvis statu and merely gotta go back and forward it’s actually quite hard. Quite taxing for that load standing feature, okay, so that’s. The first thing you do so you shouldn’t get any knee pain with that because you’re not moving in need all right and your practise, your VMO, to get a bit of static control, your training, a lot of glute static dominance, and that structures That basi for you to be able to go okay, I can get down it and I can laden and wait bear so the second level will level 1 duty. Two is the regression where you go to the same position, but you move into the position and then you move away okay, so you steps down, but I’m not allow that knee come forward. So I’m moving more of the trendies of doing more glute succeed that I am knee work now. Of direction, your glutes are going to get stronger than your knee at this degree, but you have to because if you’ve got knee aching, you’re. Currently, there knee go forward, so it’s better designed to strengthen the trendy, do that stronger white-hot and give the knee gradually stronger and while there are encompass and gets better, then you can move into stage two which is going from the step down regression like That to actually letting that knee be forwarded, so I’m in more of a regular hunker predicament. So if you imagine like, if I was in a squatting okay, I’m doing the same thing, but I’m just doing it on one leg: alright, and you can call it a one legged hunker if you like, but we call it a step down Because that’s, the free movement of persons where develop is their ease, injure ensure and then coming back up, so we’re not actually stepping up okay, we’re stepping down and then returning , no and just letting that knee come forward. Now you can choose how much your net knee comes for you can. If you’ve got a little bit of aching later coming for Livermore, so you sit below the ache and as you get better and that improves you can get that knee going forward and forward and forward and tell us the right inclination, just like you would Do in a squat all right now, you’re level. Three, all you need to work on is putting some sort of resistance to the movement of the knee. I don’t mean lading the body there -‘s no spot putting weights on until you ,’ ve worked on the lateral component of it. So getting a stripe like this and putting it around got God to see the breast knee, but it’s the outside of your knee okay. So at the outside of your knee and you’re going to stand on that leg and then try and balance and again I’ve got to try and continue my knee on the outside of my toe all right and then the band is trying to Pull me in, I’m trying to find it, so I needed that will stir you work hard now and these new challenges me laterally. So when I go in to step down okay, I’m trying to resist the band, and that gives me more manipulate right up here. More limit, duty that I need to do is that’s about the control of the knee. Now that I’ve got the backbone up to handle the squad datum, he’s got the strength up before and now I’m going to work on my power with a better resist laden, all right and then you’ll, verify on rank four. We go to a BOSU, I mean you can use the wobble committee or a BOSU doesn’t really matter, and this is really working on a lot of motor control now, so we build our forte and a little of control there, and then we sharpens precisely On power at the end stage right because you know you can do all the squats you like to get the strength up higher and higher, but you still got to work on control for the best rehab and your knee so offset on there and the same thing Knee on the outside of your toe stepping down tapping the floor coming back up and notice, I’m not put heavines through my back leg. I’m keeping the weight on the BOSU and I’m trying to keep it level. Doesn’t matter. If it moves a little bit as long as my knee remains quite stable, doesn’t roll in okay and same with my trendy again, keeping that hip nice and position , not making it dip down and coming back up and that’s it

Low Back Pain Clinical Practice Guidelines: Part 1 Overview
admin123 0 Comments Back Pain CHRONIC PAIN
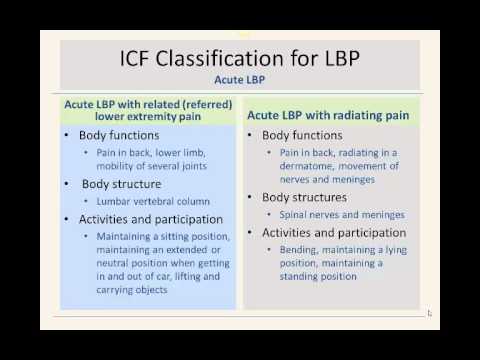
hello my name is Adam Yoder I’m a current gim fellow in training welcome to this introductory presentation on the clinical practice guidelines for low back pain this guideline is produced by the orthopaedic section of the apt a in conjunction with the World Health Organization this presentation is a very brief overview of the clinical practice guidelines for low back pain more in-depth information will be presented in part two I hope you find this information a value in your current clinical practice the apt a and orthopedic section began a process to develop clinical practice guidelines based on the latest evidence for common clinical syndromes the purpose of the clinical practice guidelines are to enhance clinical practice patterns by assimilating and appraising the latest clinical evidence for management of patients with low back pain the purpose is also to stimulate further research in areas where there is little evidence to help guide clinical practice please visit the orthopaedic section of the APTA for further information on the clinical practice guidelines this slide is taken directly out of the document and on this slide you’ll see there are several purposes to the guidelines that have been listed below obviously one is to enhance clinical practice the other is to give researchers better ideas of what to further research in areas that we don’t know very much about low back pain another reason is to provide information for payers and claim reviewers regarding physical therapy so as you can see there’s many different reasons on why that the guidelines have been produced and why the APTA is taken on this initiative so the orthopedic section looked and talked to specific experts in low back pain to help develop the clinical practice guidelines and the panel of experts were sort of given several initiatives on what to research and want to discuss the first thing was to look at look at and identify body function structure activity limitation and participation as described by the World Health Organization’s IFC guidelines then they wanted to categorize patience into movement impairment patterns to base interventions in these categories were all kind of determined through the IFC guidelines based on the body function structure activity limitation and participation deficits then after after looking at those and assessing the movement impairment patterns they looked at the end of the best interventions to fit those categories and then they determined how much evidence existed in treating those impairment patterns the lead author then assigned other authors or other experts to subcategories within low back pain such as classification examination and intervention to search the literature typically each author was designated an area where they were more of a specific expert such as the classification or specific interventions each author then independently searched the literature MEDLINE cinahl cochrane database to find the best available evidence the articles were then compiled by the authors and were scrutinized and then it was determined how relevant they were to their area that could eventually be included in the document these individual articles were then graded according to the criteria described by the Center for evidence-based medicine there is a website that you can go to for the Center for evidence-based medicine that talks about the different levels of evidence and studies that we do have level one evidence was from a high quality diagnostic study these are typically randomized controlled trials level two was evidence obtained from a lesser quality study they could be randomized controlled trials but or maybe a little bit weaker in their standard such as their randomization or blinding the third was case control studies or retrospective studies fourth would then be a case series and then five would be expert opinion that was how each individual article was graded by the panel of experts after individual articles were graded they were then pooled and then the overall strength of the evidence in a particular particular area was was graded so for example grades of recommendation and the clinical practice guidelines could be a strong evidence so if there were several level one and or level two studies they would then most likely grade the overall recommendation on strong evidence be moderate evidence was a single high quality randomized trial or several level two studies weak evidence see was a single-level – or could be level three and four studies and could be statements of consensus or expert opinion d conflicting evidence may have higher quality studies but some of these studies may disagree with with each other on their conclusions so then with conflicting evidence they would be given a D grade a theoretical foundational evidence this is going to be evidence from lower studies such as animal cadaver studies or based on models basic science an expert opinion F recommendation would be based on clinical experience or guidelines from development teams I just want to make a comment here about the intent of the clinical practice guidelines it should be noted that the lope back-pain clinical guidelines are guidelines they’re not intended to serve as the standard care of medical care and physical therapy adherence to guidelines will definitely not ensure a successful outcome with each and every patient in managing patients physical therapists should include patient values expectations and preferences in their management another key aspect is that clinic clinicians should also adhere to sound clinical reasoning skills and should not blindly follow the guidelines without clinical reasoning skills and considering the patient in front of them one large area of the clinical practice guidelines for low back pain was developing a classification system for patients the apt a looked at the World Health Organization’s framework for determining disability and function throughout the world to help create a classification scheme for patients with low back pain they really looked at two domains they looked at the body structure such as the structure of the back which would be the low back the hip the pelvis what was the structure involved and the function of the area what is the functional what are the functions that those areas that undertake and the other area was activity and participation how do patients classified in a certain area how does it limit certain activities and participation more information can be found about the classification scheme by visiting the World Health Organization’s website the first classification is acute low back pain with mobility deficits so this is typically a patient who presents with problems with mobility and the body functions under the body functions category could be pain in the back thigh and the mobility of joints the body structure is then the thoracic lumbar or pelvic joints and this may limit them with activities and participation such as bending so this is the first classification it may also look similar to the treatment based classification manipulation or mobilization category the second category is very similar to the first category low back pain with mobility deficits however this specific classification is different from the first and that it is considered sub acute meaning the duration of the symptoms have simply been going on longer than the acute low back pain again the body functions could be a pain in the back buttock and groin there will be modal mobility deficits possibly of several joints vertebral segments hip joints thoracic are all areas of mobility deficits and that this does involve thoracic lumbar pelvic joints as well as the muscles and ligaments and again the main activity and participation limitation is going to be bending again similar to the treatment based classification of manipulation mobilization the next category is acute low back pain with movement impairments this classification could also be looked at very similar to the stabilization category in the treatment based classification if you’re familiar with that body functions pain in the back or lower limb and control of complex voluntary movements so the structures typically involved are going to be the muscles of the trunk pelvis and hip region activities and participation limitations could be shifting bodies center of gravity maintaining a specific body position and maintaining good alignment of the trunk and pelvis the next classification is low back pain with movement coordination impairments however this is now sub acute and chronic low back pain body functions are similar to the previous classification pain in the back lower limbs control of voluntary movements same body structures typically are involved such as the muscles of the trunk ligaments and fashio of the trunk the hip joint and thigh activities and participation again shifting center of gravity and maintaining alignment maintaining sitting positions may also be limited bending and completing a daily routine are all going to be activities that may be limited in these patients the next two categories are acute low back pain with related or referred lower extremity pain and acute low back pain with radiating pain in acute low back pain with referred pain again the body functions will be pain in the back lower limb and mobility of several joints it typically involves the lumbar vertebral column patience may have a difficult time maintaining a sitting position maintaining an extended or neutral spine may have difficulty getting in and out of a car and lifting and carrying heavy objects this classification may be similar to a directional preference classification scheme the next one acute low back pain with radiating pain involves pain in the back radiating in a dermatome and involves movement of the nerves and meninges so a nerve root compression or nerve root problem is most likely associated with acute low back pain with radiating pain activities and participation may have difficulty with been bending maintaining a lying position or maintaining a standing position this classification may be similar to a directional preference category or possibly a traction category the next classification is sub acute and chronic low back pain with radiating pain again very similar pain in the back lower limb and in a dermatome apat ern typically involves the peripheral nerve roots as well as the spinal column and again bending maintaining positions such as lying standing or maintaining a slump sitting such as driving in a car may also be limited in this population acute and subacute low back pain with cognitive or affective tendencies is the next category typically these patients have sensitivity to noxious stimulus pain with limited range of motion and often have mental functions that are inappropriate for the amount of pain that they do have the body structures that involved are typically the cortical lobes and midbrain diencephalon and brain stem these patients typically have a difficulty completing daily routine and managing diet and fitness and living a healthy life chronic low back pain with related generalized pain is typically a patient who has developed chronic pain or has chronic pain syndromes such as fibromyalgia there’s often a link to the brain such as the cortical lobes midbrain and is often a progression from acute low back pain with affective tendencies these patients are very difficult to manage and they often have difficulty managing their daily routine work requirements diet and fitness and how to even have difficulty with relationships and social interactions due to their pain again this this category someone who has potential fear of odin’s beliefs and other maladaptive mental behaviors this slide is taken directly out of the low back pain guidelines and is just a brief overview of the different classifications they also include the ICD codes underneath the classification so again acute and subacute low back pain with mobility mobility deficits the icd-9 icd-10 segmental or somatic dysfunction acute subacute and chronic low back pain with movement coordination impairments often considered spinal instabilities with ICD codes acute low back pain with referred pain often considered flat back syndrome or lumbago acute and subacute chronic low back pain with radiating pain lumbar radiculopathy neuritis lumbago with sciatica so you can see the different categories there that have been outlined and the different ICD codes that go along with that please take a moment to orient yourself to this slide there’s a lot of information on this slide basically what we have here is the classification with the ICD associations the symptoms impairments and the primary intervention strategies that should be included that are recommended by the panel of experts so our first category acute low back pain with mobility deficits symptoms typically acute low back pain buttock rafi pain quick onset of pain sometimes unilateral pain and often links to an unguarded or awkward movement they usually have lumbar range of motion limitations as they do have mobility deficits they may have low back and extremity symptoms the primary interventions are manual therapy procedures it’s recommended thrusts manipulation and other non thrust mobilization techniques to diminish pain and improve pain therapeutic exercises should also be implemented to maintain spinal mobility and supplement manual therapy procedures patients should also receive education to stay active to continue an active lifestyle and not to succumb to bed rest the next category is sub acute low back pain with mobility deficits they have similar symptoms as the acute low back pain with mobility deficits however these impairments typically are reproduced with end range motions and they usually will have restricted thoracic range of motion lumbar range of motion or lumbo-pelvic or hip range of motion with segmental mobility restrictions again manual therapy procedures thrust and non thrust are recommended therapeutic exercises to supplement the manual therapy and the focus should be on preventing reoccurrence of low back pain this slide discusses acute low back pain with movement coordination impairments or spinal instabilities an acute exacerbation or reoccurrence of low back pain is commonly associated with spinal instabilities these are typically younger females who have lots of motion and are very flexible they typically present with with pain with initial to mid-range spinal movements and it may produce low back or extremity pain they often exhibit movement coordination impairments such as aberrant spinal motion the recommended treatment approach is neuromuscular reeducation to help promote the dynamic stability of the spine external devices could be used temporarily to help stabilize the spine self-care and home management training strategies should be utilized to help protect the patient and they should be educated on proper posture and maintaining good spinal position the next one is sub acute low back pain with movement coordination impairments these patients now have impairments with mid-range motions that worsen with end range movements often low back and related extremity pain can be produced there’s typically a hypermobility of a spinal segment usually in the lumbar spine there may also be stiff or mobility deficits in the thoracic spine or possibly the hip region typically these patients also have diminished trunk control and strength neuromuscular re-education again should be prescribed for these patients manual therapy procedures should be incorporated where there is a loss of mobility in certain areas whether it be in the thoracic lumbar hip and therapeutic exercises to improve endurance and muscle strength should be utilized again I just want to draw your attention to chronic low back pain with movement coordination impairments very similar presentation to acute low back pain and sub acute low back pain with movement coordination impairments however it’s just more chronic or more reoccurring and typically they have pain that is worse at end range and worsens with sustained and end range motions they present with high permeability of segmental testing typically the lumbar spine again may have mobility deficits somewhere else in the region such as the thorax thoracic spine or hips neuromuscular re-education is the treatment that is recommended and manual therapy procedures and interventions should be used in areas that are identified to be hypo mobile strengthening and re-education are the key and community work reintegration training is important if they are using their spine in a way that is somewhat physical the next category is acute low back pain with related or referred lower extremity pain also known as flat back syndrome or lumbago according to the ICD codes typically acute low back pain commonly in the buttock thigh leg impairments they can present with a pain in the low back or leg that can be centralized with specific movements they may present with the reduced lumbar lordosis and they may have limited extension mobility they may also present with a lateral list or a lateral shift of the trunk typically these interventions are going to be therapeutic exercises manual therapy or traction procedures to promote centralization these patients also need education in correct positions especially in sitting neuromuscular reeducation interventions may also be appropriate for these individuals acute low back pain with radiating pain is often presented with a very narrow band of land sating pain very specific to a dermatome the patient may also experience numbness and tingling and or weakness in the leg they typically have pain with initial to mid-range movements the procedures that are recommended our education in is in position such as sitting standing walking manual or mechanical traction is also recommended a manual therapy to take pressure off the nerve roots manual therapy to the soft tissues to help relax the patient are also recommended nerve mobility exercises in the pain-free non symptom range may also be recommended the sub acute low back pain with radiating pain similar progression however these patients may also present with mid-range and worsening with end range movements they may have lower limb tension tests that are positive such as the slump or the straight leg race they may still have extremity sensory or strength reflex deficits again manual therapy to mobilize the spine manual or mechanical traction to take pressure away from the nerves or nerve roots nerve mobility exercises in the mid-to and ranges to improve the mobility of the dura chronic low back pain with radiating pain typically these patients will have problems with sustained or end range movements that put stress on the lower limb nervous system they may also begin to or also continue to have signs of nerve root involvement manual therapy interventions and exercises are recommended in these patients to mobilize the nerves and the tissue around the nerve roots patient education again is recommended especially if patients are sustaining positions such as sitting or in positions of end range stress acute or subacute low back pain with cognitive or affective tendencies are usually described as disorders of the central nervous system symptoms are acute or subacute low back pain and they may have lower extremity pain as well these patients may have positive mental disorder screens that are positive such as the highs higher scores on the fear voidance beliefs or high scores on pain catastrophizing scale they may also have signs and symptoms of depression these patients really need patient education and counseling whether that be by the physical therapist or by professional psychologists chronic low back pain with related generalized pain these patients typically do not follow a clinical pattern of mechanical low back pain they may have disorders of a central nervous system where they have more widespread pain and again these patients may be positive for screens such as depression high scores on the fear voidance beliefs or high scores on the pain catastrophizing scale these patients again really need education and counseling whether that be for depression or counseling for fear avoidance beliefs or pain catastrophizing behaviors these patients may also benefit from low intensity prolonged aerobic exercise activities these patients will typically not respond well to higher intensity exercises they me they may need lower more graded exercises now that we’ve talked through the classification system that’s proposed by the expert panel and the Jo SPT guidelines for low back pain I want to go through a summary of recommendations on other areas that are important in the management of low back pain the first areas risk factors of low back pain the current literature and the panel did not find a specific definitive cause for the initial onset of low back pain what they found is that low back pain is often multi-factor ‘el and it can be specific to certain populations this is based on be moderate evidence the clinical course of low back pain is typically defined as acute subacute Riya current or chronic in nature and given the disability associative low back pain and the high medical cost of low back pain interventions should be directed towards preventing reoccurrences and chronicity this is based on theoretical foundational evidence we’ve already discussed fairly in-depth of the classification system that’s proposed by the panel in the Jo SPT guidelines there are other classification systems available such as the MD T or Mackenzie approach and the treatment based classification proposed by Fritz it is recommended by the panel that classifying patients into categories has benefits typically these patients are classified based on their signs and symptoms and then matched to the best treatment based on their signs and symptoms this is based on moderate evidence and this will be discussed more in depth in part 2 of this presentation differential diagnosis is a very crucial part of being a physical therapist it is important that physical therapists know the red yellow flags of patients that may come into their office we must know who and when to refer it’s with strong evidence that the panel recommends procedures to differentially diagnose patients based on their signs and symptoms it’s recommended that if patients symptoms are not resolving with treatment aimed at restoring the impairments that they be referred on outcome measures such as the Roland Moore’s disability questionnaire and the oswestry disability index have been studied very significantly and are highly recommended by the expert panels it’s with strong evidence that these disability questionnaires are recommended these tools are very helpful in determining a patient’s baseline status and monitoring their status over time through the course of treatment it is also beneficial for the clinician or therapists to monitor their ability to treat and improve patients over time not only should clinicians consider self-report measures such as the Oswestry or role and Morris disability questionnaire they should also look at work capacity evaluations or activity and performance measures to determine the level of activity a patient may be able to perform this is based on expert opinion and the experiences of the guideline team as was discussed earlier manual therapy interventions should be utilized in patients with low back pain this is based on strong evidence thrust and non thrust joint manipulative procedures should be considered especially in those patients that present with mobility deficits and have acute subacute and chronic low back pain drunk coordination strengthening endurance exercises are commonly prescribed for patients with low back pain it is with strong evidence that drunk coordination strengthening endurance exercises are recommended clinicians should definitely consider these interventions in patients with sub acute and chronic movement coordination impairments they should also consider these strategies in patients that are post lumbar microdiscectomy centralization and directional preference exercises and procedures are recommended based on strong evidence clinicians should consider using repeated movements sustained movements or exercises or proceed that will promote centralization and patience typically these procedures will be used in patients with acute low back pain with referral to the lower extremity they can also be utilized in patients with acute or subacute low back pain with mobility deficits flexion exercises have often been prescribed for patients with low back pain as well however we have weak evidence to support the use of flexion exercises in isolation however flexion exercises can be beneficial when packaged with manual therapy strengthening exercises in potentially nerve mobilization procedures in patients that are elderly or who present with chronic radiating pain or signs and symptoms consistent with spinal stenosis there is weak evidence to support lower quarter nerve mobilization procedures however clinicians should consider using lower quarter nerve mobilization procedures in patients with acute and chronic low back pain and radiating pain traction has typically been an intervention that causes some controversy among physical therapists and it’s with conflicting evidence that traction is recommended it is not recommended with patients with acute or subacute non radicular low back pain if mechanical traction is used it should typically be used when there are signs of nerve root compression or if there’s peripheral ization of symptoms or a positive cross straight leg raise patient education and counseling is recommended based on moderate evidence for patients with low back pain patient education and counseling should can that are affirming the patient that the human spine is very strong they should also consider using neuroscience education that explains the patient’s pain perception they should continue to affirm the patient of the favorable prognosis of low back pain they should continue to help support them and using active coping strategies and they should really reassure the patient that they should reactivities and focus on function not just pain it is not recommended to include in-depth patho anatomical explanations to patients as this may create an increased amount of threat or fear to them progressive endurance exercises and fitness activities are recommended based on strong evidence moderate to high intensity exercises such as aerobic and strength training should be utilized for patients that have chronic low back pain without generalized pain it’s recommended that those that have more of generalized pain would do better with lower intensity submaximal fitness and endurance activities more graded low level activities are recommended for patients with generalized low back pain again I just want to emphasize that these are just guidelines and the evidence and expert opinion can change over time I do encourage you to classify and use inner interventions based off classifying patients matching treatments to their presentation and I also want to encourage you to consider using patient values and your own personal clinical reasoning from previous experience as well as the evidence in your approach to treating patients with low back pain again thank you for listening to part one a more in-depth presentation on specific articles and evidence will be presented in part two I thank you very much for listening and we’ll see you in part two


Reduce neck and shoulder pain in a one arm row / pull | Feat. Tim Keeley | No.23 | Physio REHAB
admin123 0 Comments Back Pain CHRONIC PAIN
okay today and we are looking at trying to get you working on the correct row post for your shoulder blade or your scapula so a lot of parties are having troubles when they row or when they do an forearm draw they’re doing the wrong things with their slipshod auto-mechanics and that can be due to pain to be witness to the four practices bad muscle govern today we’re going to try and support you how to use exerts to try to improve their control what their power needs to be like so a lot of time beings have sorenes down now the old-fashioned cervix ache from from computers or their training too hard and we accompany a lot of people with pain into the rhomboids and into that levator SCAP meet your sketch and what it tends to do is it tends to muck up their shoulder move and they tend to pull incorrectly and they tend to push incorrectly now this episode is about the pulling movement clearly we’re doing we get beings doing a lot of serratus movement and press fluctuation but we’re talking about the pull advance so with plucking what we want to focus on this with the sequence is Magnus sure you’re doing getting your shoulder blade plucking back correctly been using it rhomboids you’re using lats but uttering sure you access the lower bunkers to keep the shoulders stable most of time people attract and they pluck and they hoist and they use their upper trap to try and compensate because they’re massive baits aren’t working or “theyre using” this cire their levator SCAP to pull upwards and they can plead to a lot of difficulties when you rogue with a lot of neck pain and a lot of shoulder pain especially in the figurehead of the shoulder so first things firstly we’re going to try and I’ll testify you what the chastise action is for the shoulder route when you attract and then we’ll show you some practices so if you imagine what you’re trying to do when you draw when you move back with your shoulder bone has to come back first okay so shoulder bay comes back and as I pull back I’m exploiting the long committees but I’m trying to getting my fright catch activated so my shoulder baits sitting down I gathered it right back and then I’m going to pull through with my appendage preparing sure though when you pull through what you’ve all had to do is then rotate because I’m letting got to go so I’ve got to pull back hold it back squeeze out there pull round and then when I return it’s just a reverse flow so return the appendage to a dupe most movement and then get the shot of protech for okay so if we can start off on usage and now he only grab a pole could be a door jamb can you think what I require you working on is starting and then stay moving out you can go high-pitched and which axis in the bottom I’ll check that same crusade so you pull back it’s a style of shift so this is scapular rows consuming a saloon and you notice this is a closed chain position so it accesses a lot more stabilizers then then doing an open chain so that the closed chain position so I’m doing a scapular sequence so I’m just pulling my shoulder craft back and there’s my shot of a drags back I’m putting my torso forward right made to ensure that I don’t go on elevate and access my upper bunker to do a bit operate I’ve gotten try prevent my my distance between my ear and my shoulder quite little okay so drawing back pinching back and then not just dropping I’ve got a gradually release that a shorter way forward so that’s just scapular right okay with the bar really good want to start and then you can start doing with a band so this is more of an open bond exert so I’m now working on trying to do the same movement but restraining my person still so if this movement now I’m going from there and it’s just the shoulder bag that’s a very vulnerable exercise pretty easy what you’ve got to try it’s teaching you though to do scapular push precisely when you travel okay most the time you’re used to pulling so when you pull back you don’t want to start beating your shoulder so try and forestalled that so you by the right bank that I tell about it and then release forward again okay so scapula back and then forward again now to join combine that together you want to do a one-arm right and we can only use a exhibition bet if you’re a big week you’ve got a bit of pain I simply show go down to one but I’m expend 2 day so when you pull through now so we’re going to use the idea of make kept in a row so it’s row back then feeds your appendage for now as I come through I’m still pulling back I’m not countenance it go okay so I still want to get that last few kind of 1020 the Greens have didn’t have the traction back and offsetting sure I’ve got a decent distance between now and my shoulder so I’m not elevating I’m exerting my lower check and Matt’s gonna out your back here so stop that core on now when I’m back here I’ve got to try and stop my shoulder room back as I return the arms and don’t pop the shoulder move forward now keep your shot of a back as I return the forearm and then there’s a shot of a project quarter so that’s the movement that you guys need to be doing whenever you do any gathering with rowing pitch-black pull down stats I think it’s manufacturing sure you bounce the road pull through return return and I like to do this something finger on the back so thumb on the back of that shoulder bait so I can feel when my shoulder like this my finger pull through now obstruct my shuttle bay on my thumb and don’t mean it pull away my paw it’s a really nice little tube you can get that sort of shorter boat on your finger so as it comes back strokes your finger push your arm through and then keep it there until you need to release and let it go so this is one R one and row and then we can go okay what about pull down so if we go to something higher appended imagine like you’re doing a one-armed pull down like on a cable machine or we’re doing lat pull-downs this is going to help you perfect that move through your shoulder so when you do pull down when the load gets any when it starts get heavy you don’t go and do this because we find it when people do lat pull-downs the heavier the consignment when they pull down they start you read those shoulder blades rising up so we’ve got to get you going draw those shoulders down and then pulling through and to be maintained down and then as you return you’ve got to keep them down for the first part of it and then construct the rest far too many people make them release very immediate okay so this is where you have to go back higher and again one arm at a time because you can access one forearm at a time that’s way better to learn so if we came from here you down it now if you want to go lower down into one me shoulder back down pull right through better here’s the quirk impede that shot away back exploiting those mower racetracks down the back here and then release forward okay recur pull down pull through hold it down there and secrete sport and this is great for determining what with all those problems but beings are going sorenes anteriorly in the shoulder when they pull through that missile rollings for intensive want to roll out the seam when they pull through and they’re getting ache in the front so sick that a little more properly and likewise facilitates with parties going anguish in the back here where they’re overusing rhomboids overusing upper traps overusing levator SCAP and not accessing those lower trad muscles so start working on that likewise check out our lower trap exercisings that we have on on the videos and our serratus interior for the pressing work


How to Squat Safely and Correctly with a Back Injury | Feat. Tim Keeley | No.71 | Physio REHAB
admin123 0 Comments Back Pain CHRONIC PAIN
all right we’re here today with Nicky and we’re demonstrate you how to do a squat properly and safely when you’ve got a dispersion and how to prevent any disc injury so with Nikki she’s got a current put and when she squats we’ve got to make sure she doesn’t get below what we call a break point so Nick if you precisely show us like a squat for me and we’ll just go side on what we want to make sure if she doesn’t do that but went connection form thing and so a lot of people this sort of degree will be 90 units so she goes need lower than that can you see that what happened there so if you come and I can have a look at this she goes from at this is she’s also a little very widened at this extent as well which we’re going to fix as well but when she descent lower did you see how that opens up there now what she’s doing she’s not even actually at 90 degrees hitherto down now they’re now at that point she’s actually rounded in now which is bad for her disc prominence so come on back up again because then she goes into extension which kind of gleams the as there and she comes up again so for this one for her safety-wise and for anyone who’s got a disc bulge and wants to prevent any back ache as you can go below the target where you’re going to lose neutral prickle so at that point there she can’t make that low-toned now for some people they’ll be able to go lower than that they’ll be able to go right to 90 severities because they’ve got accumulations of range in the trendy they’ve got a really good core stability here they don’t lose any neutral backbone but for her she needs to be very aware and look in the mirror about her position so you see that neck so if you come down again for me – she needs to go – woo come back up and she need to get used to where that situation is okay because if she goes in lower she goes into flexion she’ll then posterior projection that saucer and then reinjure herself so she’s got to work on that the other thing she’s got to work on is she charities being hyper diversified here all right so this position here needs to actually become a bit of neutral now I don’t mean go into flexion I make she exactly needs to stay in neutral so she’s got to really hold the line interior with her core there and when she hunker she’s got to keep it on she wants to just till she wants to incline this pelvis like that to kind of squat because she wants to behold her sticker increase instead of go into flexion but that becomes really bad when she gets down the bottom so she’s got to learn can I regard neutral in the backbone and deflect at the hips so the hips have to go down and back so try that for me neck there you go that’s better and then she stops Laura Laura like she still has to watch her burst top she stops her neutral backbone just so much harder right and then come back up with hip postponement so when she comes back up she doesn’t have to then tuck a slacker under it’s actually in neutral so the gimmick is start a neutral and go very slowly down expand the trendies backwards and down into that position that she maintains initial don’t go below that breakpoint and glance the butt and then when she comes back up he’s got an alia to extend and then she comes back neutral and that’s it hard to practice and she’s just make the body weight of mine because it’s if you try and introduced stockpiles of heavines on there she’s going to one go into an age-old structure but she’s also just going to load the prickle which we don’t want okay so for her it’s going to be really hard for her to try and try that again with a table it’s going to try it it’s going to be hard for her to do a back squat in that position because if occur in the shift if she tries to a back squat what happens is you tend to extend through your backbone up that so she’s going to find it relatively hard to keep a neutral when she goes down so you try that for me yes just kind of find it see that did you see that so she went straight into extension that point there come back up again so I don’t really like this for knee hurting so you wouldn’t elevate someone’s ends if you had patellofemoral suffering you wouldn’t do that but for her what we can do as long as those feet are apart she prevents her knees apart we can elevate her heels to help her with her spinal slot when she hunker with the intention that you’re going to take these sheets away at some object okay peculiarly if she has knee pain we’re not going to use them but now try that for me and you’ll find that she is able to maintain a better form there’s that but Winkie so again let’s try that again this is where hands-on helps a little bit so neutral she sits down and back comprised hold chase and then come back up and I’m just pas it with my hands is an attempt restrain her a neutral earn her be into the trendies the most try again for me attend didn’t do that by yourself and she’s a little bit too upright do you see that so we’ve got to try and get her directions of her upper figure the same as shin okay so try that again for me forward North upper body that’s a bit better we’re getting there chase and then come back up and bummin yeah okay so this is how we learn to try and get a better and better squat what I would do with her though to meet things even better as you were doing a front hunker so front hunker the refuge the bar so we better to rub her you start off with a kettlebell there you go now that’s ten kilos with her times difficulty one-tenth time who does trouble ten kilos is okay I probably wouldn’t go to twenty this stage just straighten your paw up for me in here that’s it alright so from here because the way from the front she can then concentrate on what’s going on with their sticker here so try that again so reciprocal backbone sit back hold push back up I’m forward so make sure you don’t fold the projectile under that’s missile forward so you extend the hip go again fine good and come back up and again she’s maintaining still a quite an upright spine we’ll get that angle forward a little bit better as we go but that’s looking really good now tips for her is to so she can see what she’s doing she needs to then vanish line-up onto the mirror and realize her own sticker and make sure that’s all correct but that’s great okay okay we’ve practised a little bit so show us again when you no need to do and she’s using now the mirror slope on and what she’s going as method better proficiency now which he watches it and now she’s got that excellent slant of back and shin together she’s got a knees wide okay she’s got a feet latitude knees wide she doesn’t want to be like this okay go again and she’s worked out how to not but gleam and continue a neutral spine not be too upright keep it forward a bit but likewise she’s worked out how to not extend here she’s worked out how to extend at the hips and keep the spine in neutral so she’s before she was sort of sitting her bum outwards now she’s holding here and now she’s worked out that you can bend here and being now squat down to fall in and those the two points of fulcrum and then this will naturally come down and you’ve got that perfect I live in there and yes we’re up on a sheet as you carp again and when she’s looking left it’s really hard to hold a load so you practice with a reflect with no weight so you’re not sort of wrecking your cervix with a heavines and then as you get the form right then you can add the value as you get better score stability better awareness of hip pinch now take the plates away

