Tag: Low Back Pain

Back Pain: KOSMODISK® Dec 2011
admin123 0 Comments Back Pain CHRONIC PAIN
-[ David] One of the great things about InDesign is that it’s so rich, so deep that there’s always more to learn. If you want to go deeper with InDesign, I have several recommendations. First check out the website that I facilitate ranged, CreativePro.com. “Hes also” the new dwelling for InDesign Secrets. There are thousands of gratuities and stunts and more every week. Plus we have a free InDesign podcast, live online incidents and more. If you sign on for a payment body, you’ll get our brochure “InDesign Magazine” every month. This is a great resource written by InDesign experts all over the world. It’s distributed as a PDF and you can download a free inquiry issue from CreativePro. If you use InDesign for professional creation, I definitely recommend you check out the InDesign Conference, which is part of CreativePro week. Of trend, you should definitely search through the online training library to find more InDesign entitlements. For instance, search for the “InDesign Secrets” title that I do with Anne-Marie Concepcion. It’s chock full of cool InDesign gratuities. Want to go deeper into any of specific topics I discussed in this course? Then check out my other entitles, including “InDesign: Data Merge and Database Publishing, ” “InDesign: Working with Photoshop and Illustrator, ” or “InDesign: Color Management.” Finally, please follow me on LinkedIn or Twitter, and also check out the InDesign Secrets radical that I help manage on Facebook. Thank you for coming along with me on this mad journey through Adobe InDesign. I hope you enjoyed the trip as much as I have. Sure, InDesign is an industrial fortitude motif and production tool, but it’s also a lot of fun. Enjoy playing with it. After all, playing with any software is the best way to learn it. Have fun and joyful InDesigning.is constant back anguish and stiffness forming your life lamentable for 20 years Cosmo disk has been helping back soreness sufferers looks just like you 2 million people have exercised Cosmo dis worldwide the unique shape of the Cosmo disc system of ribs rubs your spine like a healer you with soothing pressure you receive constant rub to the related expanse it’s cozy simple and effective you could feel good again and it’s only 149 95 say yours now at Cosmo viscom speck au or request 1 301 5 to double for 9.

Low Back Pain Clinical Practice Guidelines: Part 1 Overview
admin123 0 Comments Back Pain CHRONIC PAIN
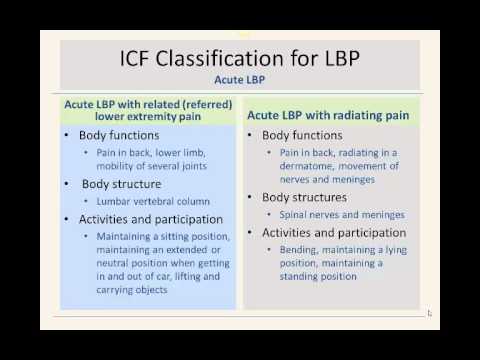
hello my name is Adam Yoder I’m a current gim fellow in training welcome to this introductory presentation on the clinical practice guidelines for low back pain this guideline is produced by the orthopaedic section of the apt a in conjunction with the World Health Organization this presentation is a very brief overview of the clinical practice guidelines for low back pain more in-depth information will be presented in part two I hope you find this information a value in your current clinical practice the apt a and orthopedic section began a process to develop clinical practice guidelines based on the latest evidence for common clinical syndromes the purpose of the clinical practice guidelines are to enhance clinical practice patterns by assimilating and appraising the latest clinical evidence for management of patients with low back pain the purpose is also to stimulate further research in areas where there is little evidence to help guide clinical practice please visit the orthopaedic section of the APTA for further information on the clinical practice guidelines this slide is taken directly out of the document and on this slide you’ll see there are several purposes to the guidelines that have been listed below obviously one is to enhance clinical practice the other is to give researchers better ideas of what to further research in areas that we don’t know very much about low back pain another reason is to provide information for payers and claim reviewers regarding physical therapy so as you can see there’s many different reasons on why that the guidelines have been produced and why the APTA is taken on this initiative so the orthopedic section looked and talked to specific experts in low back pain to help develop the clinical practice guidelines and the panel of experts were sort of given several initiatives on what to research and want to discuss the first thing was to look at look at and identify body function structure activity limitation and participation as described by the World Health Organization’s IFC guidelines then they wanted to categorize patience into movement impairment patterns to base interventions in these categories were all kind of determined through the IFC guidelines based on the body function structure activity limitation and participation deficits then after after looking at those and assessing the movement impairment patterns they looked at the end of the best interventions to fit those categories and then they determined how much evidence existed in treating those impairment patterns the lead author then assigned other authors or other experts to subcategories within low back pain such as classification examination and intervention to search the literature typically each author was designated an area where they were more of a specific expert such as the classification or specific interventions each author then independently searched the literature MEDLINE cinahl cochrane database to find the best available evidence the articles were then compiled by the authors and were scrutinized and then it was determined how relevant they were to their area that could eventually be included in the document these individual articles were then graded according to the criteria described by the Center for evidence-based medicine there is a website that you can go to for the Center for evidence-based medicine that talks about the different levels of evidence and studies that we do have level one evidence was from a high quality diagnostic study these are typically randomized controlled trials level two was evidence obtained from a lesser quality study they could be randomized controlled trials but or maybe a little bit weaker in their standard such as their randomization or blinding the third was case control studies or retrospective studies fourth would then be a case series and then five would be expert opinion that was how each individual article was graded by the panel of experts after individual articles were graded they were then pooled and then the overall strength of the evidence in a particular particular area was was graded so for example grades of recommendation and the clinical practice guidelines could be a strong evidence so if there were several level one and or level two studies they would then most likely grade the overall recommendation on strong evidence be moderate evidence was a single high quality randomized trial or several level two studies weak evidence see was a single-level – or could be level three and four studies and could be statements of consensus or expert opinion d conflicting evidence may have higher quality studies but some of these studies may disagree with with each other on their conclusions so then with conflicting evidence they would be given a D grade a theoretical foundational evidence this is going to be evidence from lower studies such as animal cadaver studies or based on models basic science an expert opinion F recommendation would be based on clinical experience or guidelines from development teams I just want to make a comment here about the intent of the clinical practice guidelines it should be noted that the lope back-pain clinical guidelines are guidelines they’re not intended to serve as the standard care of medical care and physical therapy adherence to guidelines will definitely not ensure a successful outcome with each and every patient in managing patients physical therapists should include patient values expectations and preferences in their management another key aspect is that clinic clinicians should also adhere to sound clinical reasoning skills and should not blindly follow the guidelines without clinical reasoning skills and considering the patient in front of them one large area of the clinical practice guidelines for low back pain was developing a classification system for patients the apt a looked at the World Health Organization’s framework for determining disability and function throughout the world to help create a classification scheme for patients with low back pain they really looked at two domains they looked at the body structure such as the structure of the back which would be the low back the hip the pelvis what was the structure involved and the function of the area what is the functional what are the functions that those areas that undertake and the other area was activity and participation how do patients classified in a certain area how does it limit certain activities and participation more information can be found about the classification scheme by visiting the World Health Organization’s website the first classification is acute low back pain with mobility deficits so this is typically a patient who presents with problems with mobility and the body functions under the body functions category could be pain in the back thigh and the mobility of joints the body structure is then the thoracic lumbar or pelvic joints and this may limit them with activities and participation such as bending so this is the first classification it may also look similar to the treatment based classification manipulation or mobilization category the second category is very similar to the first category low back pain with mobility deficits however this specific classification is different from the first and that it is considered sub acute meaning the duration of the symptoms have simply been going on longer than the acute low back pain again the body functions could be a pain in the back buttock and groin there will be modal mobility deficits possibly of several joints vertebral segments hip joints thoracic are all areas of mobility deficits and that this does involve thoracic lumbar pelvic joints as well as the muscles and ligaments and again the main activity and participation limitation is going to be bending again similar to the treatment based classification of manipulation mobilization the next category is acute low back pain with movement impairments this classification could also be looked at very similar to the stabilization category in the treatment based classification if you’re familiar with that body functions pain in the back or lower limb and control of complex voluntary movements so the structures typically involved are going to be the muscles of the trunk pelvis and hip region activities and participation limitations could be shifting bodies center of gravity maintaining a specific body position and maintaining good alignment of the trunk and pelvis the next classification is low back pain with movement coordination impairments however this is now sub acute and chronic low back pain body functions are similar to the previous classification pain in the back lower limbs control of voluntary movements same body structures typically are involved such as the muscles of the trunk ligaments and fashio of the trunk the hip joint and thigh activities and participation again shifting center of gravity and maintaining alignment maintaining sitting positions may also be limited bending and completing a daily routine are all going to be activities that may be limited in these patients the next two categories are acute low back pain with related or referred lower extremity pain and acute low back pain with radiating pain in acute low back pain with referred pain again the body functions will be pain in the back lower limb and mobility of several joints it typically involves the lumbar vertebral column patience may have a difficult time maintaining a sitting position maintaining an extended or neutral spine may have difficulty getting in and out of a car and lifting and carrying heavy objects this classification may be similar to a directional preference classification scheme the next one acute low back pain with radiating pain involves pain in the back radiating in a dermatome and involves movement of the nerves and meninges so a nerve root compression or nerve root problem is most likely associated with acute low back pain with radiating pain activities and participation may have difficulty with been bending maintaining a lying position or maintaining a standing position this classification may be similar to a directional preference category or possibly a traction category the next classification is sub acute and chronic low back pain with radiating pain again very similar pain in the back lower limb and in a dermatome apat ern typically involves the peripheral nerve roots as well as the spinal column and again bending maintaining positions such as lying standing or maintaining a slump sitting such as driving in a car may also be limited in this population acute and subacute low back pain with cognitive or affective tendencies is the next category typically these patients have sensitivity to noxious stimulus pain with limited range of motion and often have mental functions that are inappropriate for the amount of pain that they do have the body structures that involved are typically the cortical lobes and midbrain diencephalon and brain stem these patients typically have a difficulty completing daily routine and managing diet and fitness and living a healthy life chronic low back pain with related generalized pain is typically a patient who has developed chronic pain or has chronic pain syndromes such as fibromyalgia there’s often a link to the brain such as the cortical lobes midbrain and is often a progression from acute low back pain with affective tendencies these patients are very difficult to manage and they often have difficulty managing their daily routine work requirements diet and fitness and how to even have difficulty with relationships and social interactions due to their pain again this this category someone who has potential fear of odin’s beliefs and other maladaptive mental behaviors this slide is taken directly out of the low back pain guidelines and is just a brief overview of the different classifications they also include the ICD codes underneath the classification so again acute and subacute low back pain with mobility mobility deficits the icd-9 icd-10 segmental or somatic dysfunction acute subacute and chronic low back pain with movement coordination impairments often considered spinal instabilities with ICD codes acute low back pain with referred pain often considered flat back syndrome or lumbago acute and subacute chronic low back pain with radiating pain lumbar radiculopathy neuritis lumbago with sciatica so you can see the different categories there that have been outlined and the different ICD codes that go along with that please take a moment to orient yourself to this slide there’s a lot of information on this slide basically what we have here is the classification with the ICD associations the symptoms impairments and the primary intervention strategies that should be included that are recommended by the panel of experts so our first category acute low back pain with mobility deficits symptoms typically acute low back pain buttock rafi pain quick onset of pain sometimes unilateral pain and often links to an unguarded or awkward movement they usually have lumbar range of motion limitations as they do have mobility deficits they may have low back and extremity symptoms the primary interventions are manual therapy procedures it’s recommended thrusts manipulation and other non thrust mobilization techniques to diminish pain and improve pain therapeutic exercises should also be implemented to maintain spinal mobility and supplement manual therapy procedures patients should also receive education to stay active to continue an active lifestyle and not to succumb to bed rest the next category is sub acute low back pain with mobility deficits they have similar symptoms as the acute low back pain with mobility deficits however these impairments typically are reproduced with end range motions and they usually will have restricted thoracic range of motion lumbar range of motion or lumbo-pelvic or hip range of motion with segmental mobility restrictions again manual therapy procedures thrust and non thrust are recommended therapeutic exercises to supplement the manual therapy and the focus should be on preventing reoccurrence of low back pain this slide discusses acute low back pain with movement coordination impairments or spinal instabilities an acute exacerbation or reoccurrence of low back pain is commonly associated with spinal instabilities these are typically younger females who have lots of motion and are very flexible they typically present with with pain with initial to mid-range spinal movements and it may produce low back or extremity pain they often exhibit movement coordination impairments such as aberrant spinal motion the recommended treatment approach is neuromuscular reeducation to help promote the dynamic stability of the spine external devices could be used temporarily to help stabilize the spine self-care and home management training strategies should be utilized to help protect the patient and they should be educated on proper posture and maintaining good spinal position the next one is sub acute low back pain with movement coordination impairments these patients now have impairments with mid-range motions that worsen with end range movements often low back and related extremity pain can be produced there’s typically a hypermobility of a spinal segment usually in the lumbar spine there may also be stiff or mobility deficits in the thoracic spine or possibly the hip region typically these patients also have diminished trunk control and strength neuromuscular re-education again should be prescribed for these patients manual therapy procedures should be incorporated where there is a loss of mobility in certain areas whether it be in the thoracic lumbar hip and therapeutic exercises to improve endurance and muscle strength should be utilized again I just want to draw your attention to chronic low back pain with movement coordination impairments very similar presentation to acute low back pain and sub acute low back pain with movement coordination impairments however it’s just more chronic or more reoccurring and typically they have pain that is worse at end range and worsens with sustained and end range motions they present with high permeability of segmental testing typically the lumbar spine again may have mobility deficits somewhere else in the region such as the thorax thoracic spine or hips neuromuscular re-education is the treatment that is recommended and manual therapy procedures and interventions should be used in areas that are identified to be hypo mobile strengthening and re-education are the key and community work reintegration training is important if they are using their spine in a way that is somewhat physical the next category is acute low back pain with related or referred lower extremity pain also known as flat back syndrome or lumbago according to the ICD codes typically acute low back pain commonly in the buttock thigh leg impairments they can present with a pain in the low back or leg that can be centralized with specific movements they may present with the reduced lumbar lordosis and they may have limited extension mobility they may also present with a lateral list or a lateral shift of the trunk typically these interventions are going to be therapeutic exercises manual therapy or traction procedures to promote centralization these patients also need education in correct positions especially in sitting neuromuscular reeducation interventions may also be appropriate for these individuals acute low back pain with radiating pain is often presented with a very narrow band of land sating pain very specific to a dermatome the patient may also experience numbness and tingling and or weakness in the leg they typically have pain with initial to mid-range movements the procedures that are recommended our education in is in position such as sitting standing walking manual or mechanical traction is also recommended a manual therapy to take pressure off the nerve roots manual therapy to the soft tissues to help relax the patient are also recommended nerve mobility exercises in the pain-free non symptom range may also be recommended the sub acute low back pain with radiating pain similar progression however these patients may also present with mid-range and worsening with end range movements they may have lower limb tension tests that are positive such as the slump or the straight leg race they may still have extremity sensory or strength reflex deficits again manual therapy to mobilize the spine manual or mechanical traction to take pressure away from the nerves or nerve roots nerve mobility exercises in the mid-to and ranges to improve the mobility of the dura chronic low back pain with radiating pain typically these patients will have problems with sustained or end range movements that put stress on the lower limb nervous system they may also begin to or also continue to have signs of nerve root involvement manual therapy interventions and exercises are recommended in these patients to mobilize the nerves and the tissue around the nerve roots patient education again is recommended especially if patients are sustaining positions such as sitting or in positions of end range stress acute or subacute low back pain with cognitive or affective tendencies are usually described as disorders of the central nervous system symptoms are acute or subacute low back pain and they may have lower extremity pain as well these patients may have positive mental disorder screens that are positive such as the highs higher scores on the fear voidance beliefs or high scores on pain catastrophizing scale they may also have signs and symptoms of depression these patients really need patient education and counseling whether that be by the physical therapist or by professional psychologists chronic low back pain with related generalized pain these patients typically do not follow a clinical pattern of mechanical low back pain they may have disorders of a central nervous system where they have more widespread pain and again these patients may be positive for screens such as depression high scores on the fear voidance beliefs or high scores on the pain catastrophizing scale these patients again really need education and counseling whether that be for depression or counseling for fear avoidance beliefs or pain catastrophizing behaviors these patients may also benefit from low intensity prolonged aerobic exercise activities these patients will typically not respond well to higher intensity exercises they me they may need lower more graded exercises now that we’ve talked through the classification system that’s proposed by the expert panel and the Jo SPT guidelines for low back pain I want to go through a summary of recommendations on other areas that are important in the management of low back pain the first areas risk factors of low back pain the current literature and the panel did not find a specific definitive cause for the initial onset of low back pain what they found is that low back pain is often multi-factor ‘el and it can be specific to certain populations this is based on be moderate evidence the clinical course of low back pain is typically defined as acute subacute Riya current or chronic in nature and given the disability associative low back pain and the high medical cost of low back pain interventions should be directed towards preventing reoccurrences and chronicity this is based on theoretical foundational evidence we’ve already discussed fairly in-depth of the classification system that’s proposed by the panel in the Jo SPT guidelines there are other classification systems available such as the MD T or Mackenzie approach and the treatment based classification proposed by Fritz it is recommended by the panel that classifying patients into categories has benefits typically these patients are classified based on their signs and symptoms and then matched to the best treatment based on their signs and symptoms this is based on moderate evidence and this will be discussed more in depth in part 2 of this presentation differential diagnosis is a very crucial part of being a physical therapist it is important that physical therapists know the red yellow flags of patients that may come into their office we must know who and when to refer it’s with strong evidence that the panel recommends procedures to differentially diagnose patients based on their signs and symptoms it’s recommended that if patients symptoms are not resolving with treatment aimed at restoring the impairments that they be referred on outcome measures such as the Roland Moore’s disability questionnaire and the oswestry disability index have been studied very significantly and are highly recommended by the expert panels it’s with strong evidence that these disability questionnaires are recommended these tools are very helpful in determining a patient’s baseline status and monitoring their status over time through the course of treatment it is also beneficial for the clinician or therapists to monitor their ability to treat and improve patients over time not only should clinicians consider self-report measures such as the Oswestry or role and Morris disability questionnaire they should also look at work capacity evaluations or activity and performance measures to determine the level of activity a patient may be able to perform this is based on expert opinion and the experiences of the guideline team as was discussed earlier manual therapy interventions should be utilized in patients with low back pain this is based on strong evidence thrust and non thrust joint manipulative procedures should be considered especially in those patients that present with mobility deficits and have acute subacute and chronic low back pain drunk coordination strengthening endurance exercises are commonly prescribed for patients with low back pain it is with strong evidence that drunk coordination strengthening endurance exercises are recommended clinicians should definitely consider these interventions in patients with sub acute and chronic movement coordination impairments they should also consider these strategies in patients that are post lumbar microdiscectomy centralization and directional preference exercises and procedures are recommended based on strong evidence clinicians should consider using repeated movements sustained movements or exercises or proceed that will promote centralization and patience typically these procedures will be used in patients with acute low back pain with referral to the lower extremity they can also be utilized in patients with acute or subacute low back pain with mobility deficits flexion exercises have often been prescribed for patients with low back pain as well however we have weak evidence to support the use of flexion exercises in isolation however flexion exercises can be beneficial when packaged with manual therapy strengthening exercises in potentially nerve mobilization procedures in patients that are elderly or who present with chronic radiating pain or signs and symptoms consistent with spinal stenosis there is weak evidence to support lower quarter nerve mobilization procedures however clinicians should consider using lower quarter nerve mobilization procedures in patients with acute and chronic low back pain and radiating pain traction has typically been an intervention that causes some controversy among physical therapists and it’s with conflicting evidence that traction is recommended it is not recommended with patients with acute or subacute non radicular low back pain if mechanical traction is used it should typically be used when there are signs of nerve root compression or if there’s peripheral ization of symptoms or a positive cross straight leg raise patient education and counseling is recommended based on moderate evidence for patients with low back pain patient education and counseling should can that are affirming the patient that the human spine is very strong they should also consider using neuroscience education that explains the patient’s pain perception they should continue to affirm the patient of the favorable prognosis of low back pain they should continue to help support them and using active coping strategies and they should really reassure the patient that they should reactivities and focus on function not just pain it is not recommended to include in-depth patho anatomical explanations to patients as this may create an increased amount of threat or fear to them progressive endurance exercises and fitness activities are recommended based on strong evidence moderate to high intensity exercises such as aerobic and strength training should be utilized for patients that have chronic low back pain without generalized pain it’s recommended that those that have more of generalized pain would do better with lower intensity submaximal fitness and endurance activities more graded low level activities are recommended for patients with generalized low back pain again I just want to emphasize that these are just guidelines and the evidence and expert opinion can change over time I do encourage you to classify and use inner interventions based off classifying patients matching treatments to their presentation and I also want to encourage you to consider using patient values and your own personal clinical reasoning from previous experience as well as the evidence in your approach to treating patients with low back pain again thank you for listening to part one a more in-depth presentation on specific articles and evidence will be presented in part two I thank you very much for listening and we’ll see you in part two

